The path to a cancer vaccine has been riddled with setbacks. Throughout 20 years of clinical trials, few vaccines have proven successful. Currently, two vaccines exist to prevent the agents that cause liver and cervical cancer, but preventing cancer from spreading remains a major challenge.
The principle of cancer vaccines is simple: leverage the immune system's response to cancer to prevent or slow the disease's spread. However, this immune response rarely has a significant impact on tumors or patient outcomes.
To date, only one effective prostate cancer vaccine exists. It works by collecting a patient's immune cells, exposing them to a cancer-specific protein, and then re-injecting them to boost immunity. This method was approved in the US in 2010 and later adopted in other countries. The vaccine extends the lives of late-stage patients by about 4 months, but it doesn't slow disease progression.
Despite this modest success, the road ahead is long, with many unanswered questions. mRNA technology has partially aided this process by addressing crucial aspects like vaccination timing and target selection.
 |
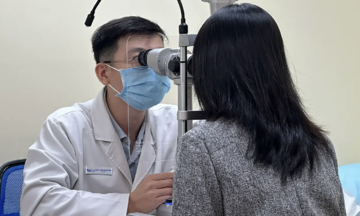
A patient in the UK receives cancer treatment. Photo: Jordan Pettitt/PA |
A patient in the UK receives cancer treatment. Photo: Jordan Pettitt/PA
A promising approach is personalized mRNA cancer vaccines. For instance, a pancreatic cancer vaccine under development in New York entered phase one trials in 2019. The vaccines were custom-made for a small group of patients, based on tissue samples from their tumors. After eight weeks, the vaccines were ready for administration.
While results are still emerging, some positive signs have appeared. Eight of the 16 vaccinated patients showed a strong immune response, and six remained cancer-free after three years. Those without an immune response experienced tumor recurrence. The vaccine is currently in phase two trials.
This research highlights a key challenge: vaccination timing. Patients receiving these vaccines already have cancer and may have undergone various treatments, impacting their immune systems. By the time cancer is diagnosed, the immune system may be too weak for the vaccine to be effective. This explains why many cancer vaccines show promise in animal studies but fail in humans.
 |
Illustration of a cancer vaccine vial. Photo: Business Today |
Illustration of a cancer vaccine vial. Photo: Business Today
Another challenge is selecting the right target. Identifying tumor-associated antigens – proteins or molecules on the surface of cancer cells that trigger an immune response – is difficult. Not all cancers express many antigens, and some antigens may be shared with healthy cells. Other antigens are invisible to the immune system.
Experts must predict whether an antigen will trigger an immune response. In a lung cancer vaccine study at University College London, researchers are using two approaches: one vaccine targets a common tumor antigen, while the other is tailored to the patient's tumor based on their genetic profile.
The team is also analyzing how the body responds to the vaccine at different stages of lung cancer. In early stages, vaccines may trigger a stronger immune response, but there are fewer antigens to target. In later stages, the immune response is overwhelmed, making it less responsive to antigens.
Despite promising results and the potential of cancer vaccines, Claire Bennett, an immunologist at University College London, notes that fundamental questions remain. Clinical trials haven’t yet yielded the same strong immune response seen with checkpoint inhibitors for some cancers.
However, the significant burden of cancer and the need for less toxic treatments than chemotherapy are driving cancer vaccine development. Vinod Balachandran, a surgical oncologist at Memorial Sloan Kettering Cancer Center in New York, believes that using a groundbreaking technology to change treatment outcomes for various cancers will strongly motivate government support.
Chi Le (According to Nature)