

A 1975-slice CT scan at Tam Anh General Hospital in TP HCM revealed severe symmetrical pectus excavatum with a Haller index of 6 (the ratio between the transverse diameter and the anteroposterior diameter of the chest, normally below 2.5). The patient's sternum was twisted at an 11.5-degree angle, the heart was compressed and displaced significantly to the left, and the thoracic spine was curved with a Cobb angle (measuring the curvature of the spine) of approximately 22.5 degrees. An echocardiogram showed pseudo-dilation of the right ventricle due to compression, and pulmonary function tests indicated reduced respiratory capacity.
According to Dr. Tran Thuc Khang, Deputy Head of the Cardiothoracic Surgery Department at the Cardiovascular Center, pectus excavatum is a congenital anomaly caused by abnormal development of the sternum and costal cartilages. Up to 20% of cases are accompanied by scoliosis. Pectus excavatum can cause scoliosis or be a comorbidity along with scoliosis in connective tissue disorders such as Marfan syndrome.
Untreated severe pectus excavatum can compress organs in the chest cavity (especially the heart and lungs), affecting respiratory function. Compression of the heart can cause mitral valve prolapse (in 20-60% of cases), leading to cardiac arrhythmias. This patient had congenital pectus excavatum but did not receive treatment until the scoliosis became severe and he experienced exercise intolerance, prompting his family to bring him to the hospital.
Dr. Khang (right) performing surgery on a patient. Illustrative photo: *Tam Anh General Hospital* |
Dr. Pham Ngoc Minh Thuy from the Cardiovascular Center explained that the ideal age for pectus excavatum surgery is between 8 and 15. At this age, the rib cage is still malleable and highly elastic, making it easier to reshape, causing less pain, and reducing the risk of recurrence. The patient underwent the minimally invasive modified Nuss procedure with thoracoscopic assistance.
The surgical team performed the modified Nuss procedure with only two small 2.5 cm incisions on both sides of the chest wall, along with thoracoscopic assistance. Two metal bars were placed under the rib cage to lift the sunken chest back to a near-normal position. Dr. Khang said this modified technique is minimally invasive, reducing the risk of damage to the heart and other organs in the chest. Combined with the erector spinae plane block (ESP) anesthesia technique, the patient recovered quickly after surgery. After 24 hours, the patient could get out of bed and was discharged after 5 days.
Individuals with severe pectus excavatum and scoliosis with a Cobb angle greater than 15 degrees require individualized consideration for chest elevation because the progression of scoliosis after surgery can either improve or worsen, according to Dr. Khang.
This teenager underwent pectus excavatum repair surgery. During follow-up appointments, his breathing difficulties had resolved, his chest was symmetrical like a normal person's, and his scoliosis had improved. The patient continues to follow the doctor's advice regarding physical activity after surgery and is being monitored by both cardiothoracic and spine surgeons.
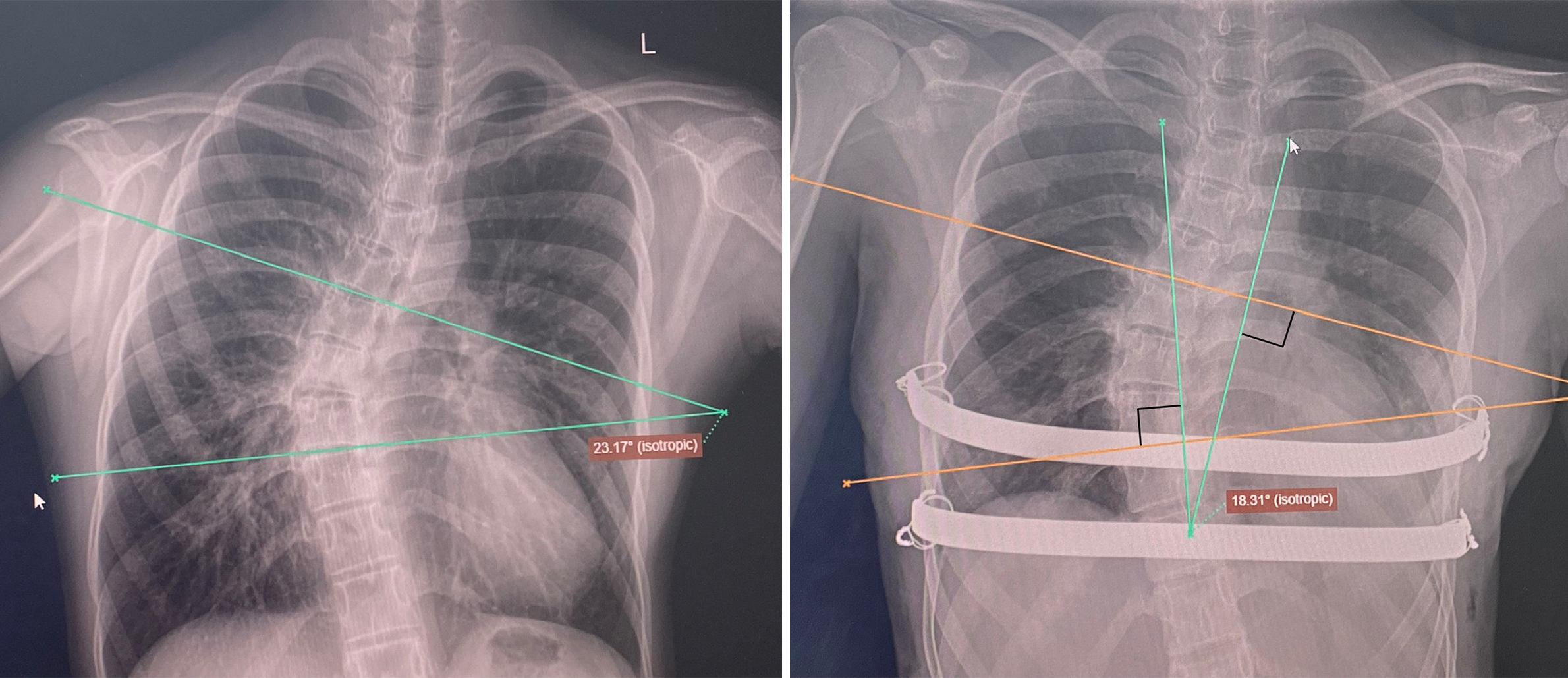 |
Pre-operative X-ray (left) shows thoracic scoliosis with a Cobb angle of 22.5 degrees, and post-operative X-ray (right) shows the support bar in the correct position, with improved scoliosis and a Cobb angle of 18 degrees. Photo: *Provided by the hospital* |
Dr. Khang stated that pectus excavatum is a congenital anomaly, but it can be completely corrected. Parents should detect it early, monitor it, and take their children for timely examinations to avoid severe progression and ensure surgery at an appropriate age.
Ngoc Chau
| Readers can submit questions about children's health here for doctors to answer. |









