On 16/5, Dr. Nguyen Huu But, a first-degree specialist in the Department of Surgical Anesthesia and Resuscitation at S.I.S Can Tho International General Hospital, stated that the child patient arrived in a deep coma with constricted pupils. A cranial CT scan showed severe brain hemorrhage, with blood spilling into the cerebral ventricles and causing acute brain compression. Cerebral angiography images also revealed a cerebral arteriovenous malformation (AVM), an abnormal connection of blood vessels that had ruptured, leading to massive bleeding.
Facing a life-threatening situation, the hospital activated a multidisciplinary consultation, agreeing on DSA endovascular intervention to embolize the vascular malformation. This procedure aimed to urgently stop the bleeding and prevent further hemorrhage before surgery.
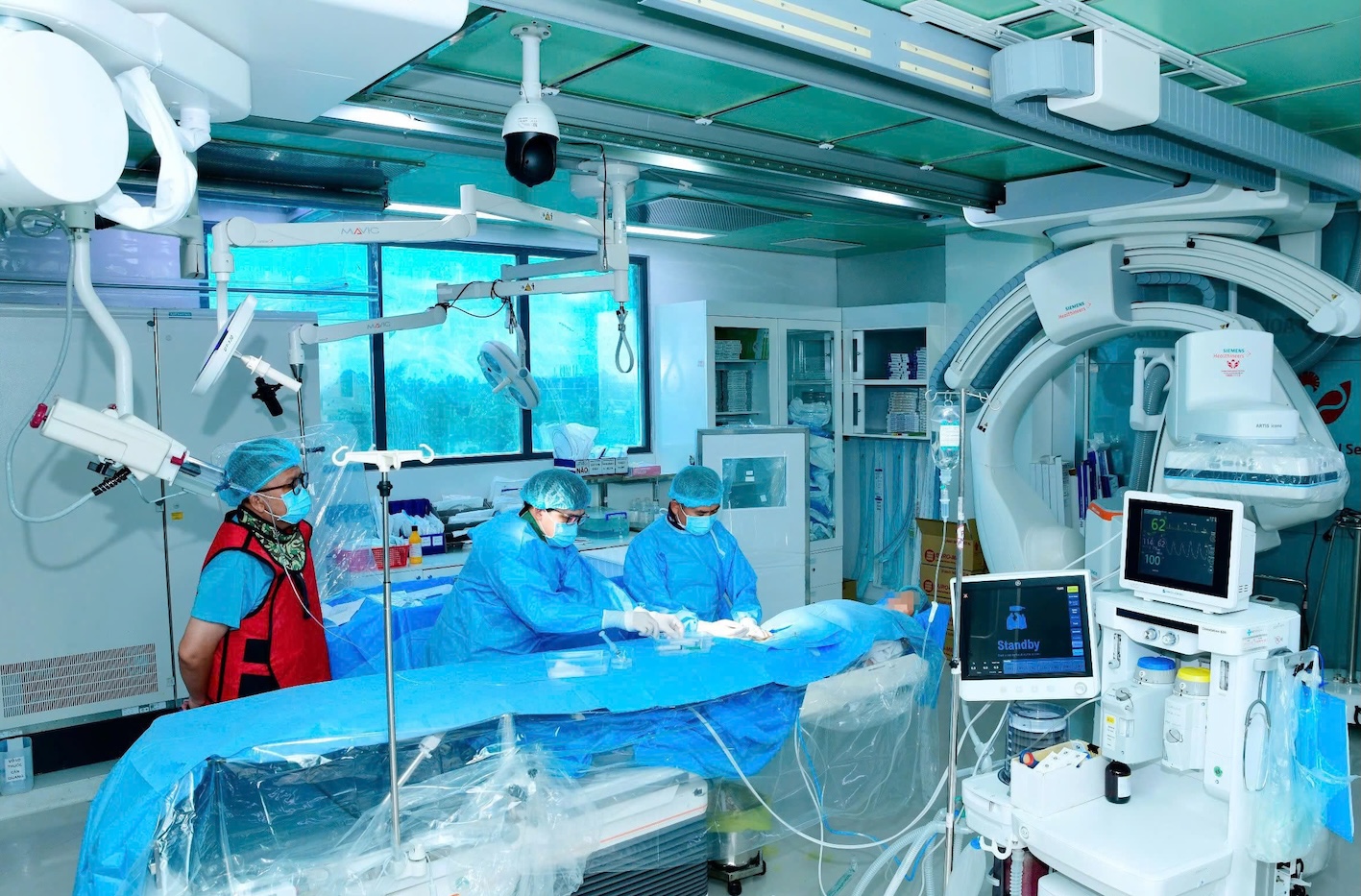 |
Doctors perform DSA endovascular intervention to embolize the brain vascular malformation for the child patient. Photo: Hospital provided |
Dr. Nguyen Luu Giang, head of the DSA unit and a second-degree specialist, noted that this was a challenging case due to the patient's young age, complex brain vascular lesion, and high mortality risk. After controlling the bleeding source, the team faced the next challenge: removing the hematoma to reduce brain compression, limit damage, and mitigate the risk of sequelae.
According to Dr. Nguyen Quang Hung, head of the Neurosurgery Unit and a first-degree specialist, the team utilized 3D hematoma localization technology, a neuro-navigation system, and minimally invasive microsurgery. These advanced techniques allowed for precise access to the lesion, minimizing impact on healthy brain tissue.
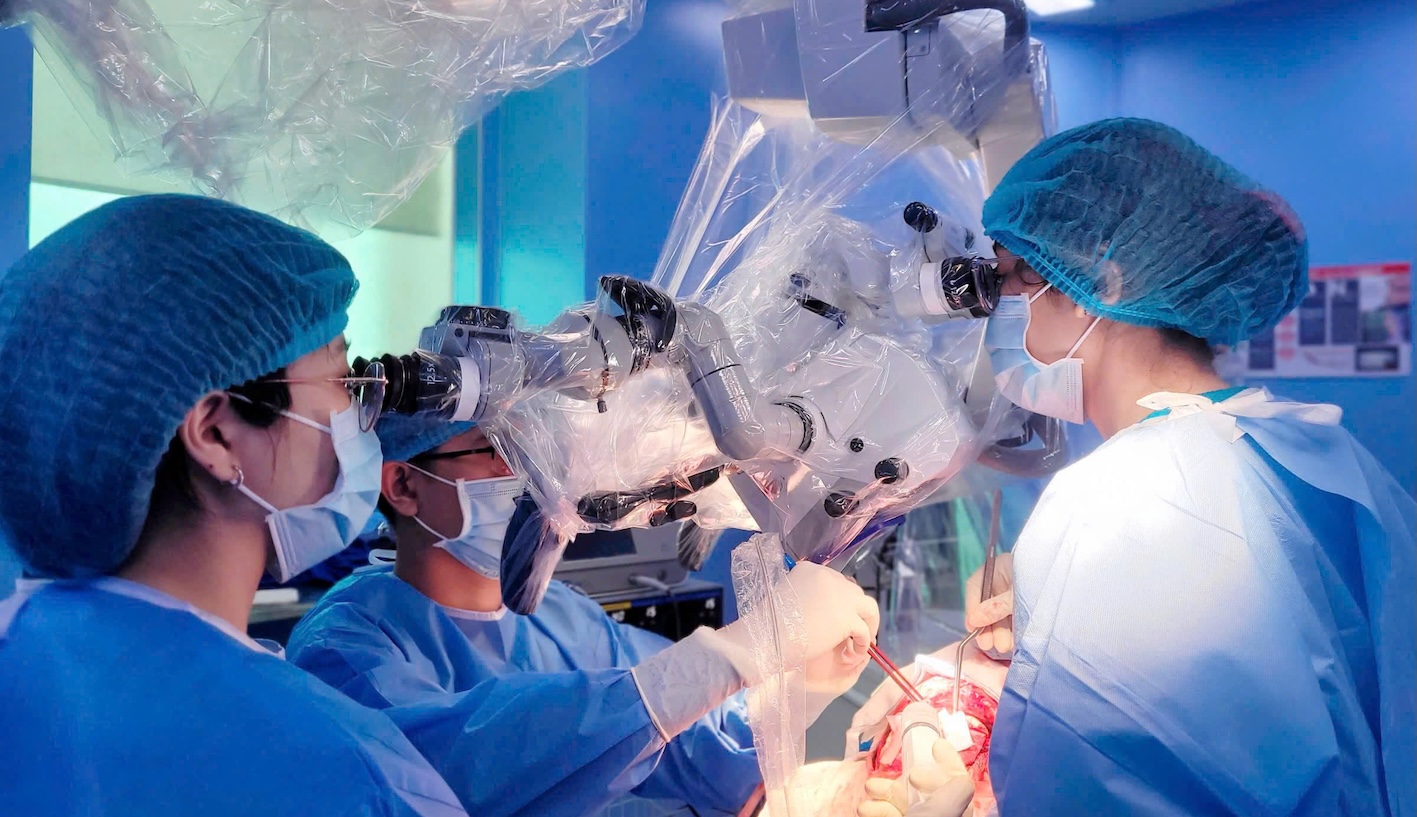 |
Doctors operate on the child patient. Photo: Hospital provided |
After surgery, the child was transferred to the intensive care unit in a sedated coma, on mechanical ventilation via an endotracheal tube. Over the next 5 days, the patient received intensive treatment, including respiratory support, anti-brain swelling measures, ventricular drainage care, infection prevention, and early mobilization exercises. Currently, the child is responsive to calls, follows commands, breathes well independently, and has been extubated, with a good prognosis for recovery.
Stroke in children differs from adults, with most cases of brain hemorrhage linked to congenital cerebral vascular malformations. This field remains a challenge for many medical facilities due to the rarity of the condition, its rapid progression, and the demand for in-depth coordination among multiple specialties, alongside modern equipment for emergency care and treatment.
Before a stroke, children may only experience transient headaches, seizures, loss of consciousness, or weakness on one side of the body, making symptoms easily overlooked. Therefore, parents should not be complacent if a child exhibits persistent headaches, facial drooping, limb weakness, speech difficulties, or unusual seizures, as these could be warning signs of a stroke or a dangerous neurological condition.
How a stroke occurs:
Le Phuong