

Aye developed severe left main bronchus stenosis as a sequela of tuberculosis treated 5 years ago. She was hospitalized three times in Myanmar due to left lung collapse, acute respiratory failure, and severe chest pain; however, she only received palliative treatment and no surgery.
Upon her arrival at Tam Anh General Hospital, TP HCM, Associate Professor Doctor Vu Huu Vinh, Director of the Center for Thoracic - Vascular Surgery, observed the patient was pale and cyanotic due to prolonged oxygen deficiency. A 3D CT scan of her lungs showed the left main bronchus was severely narrowed, like a thread, with the bronchial lumen reduced to a tiny slit, having lost its normal diameter.
"The patient has severe left main bronchus stenosis resulting from pulmonary tuberculosis sequelae," stated Associate Professor Vinh, who prescribed bronchial reconstruction surgery to improve respiratory function and attempt to preserve the patient's lung.
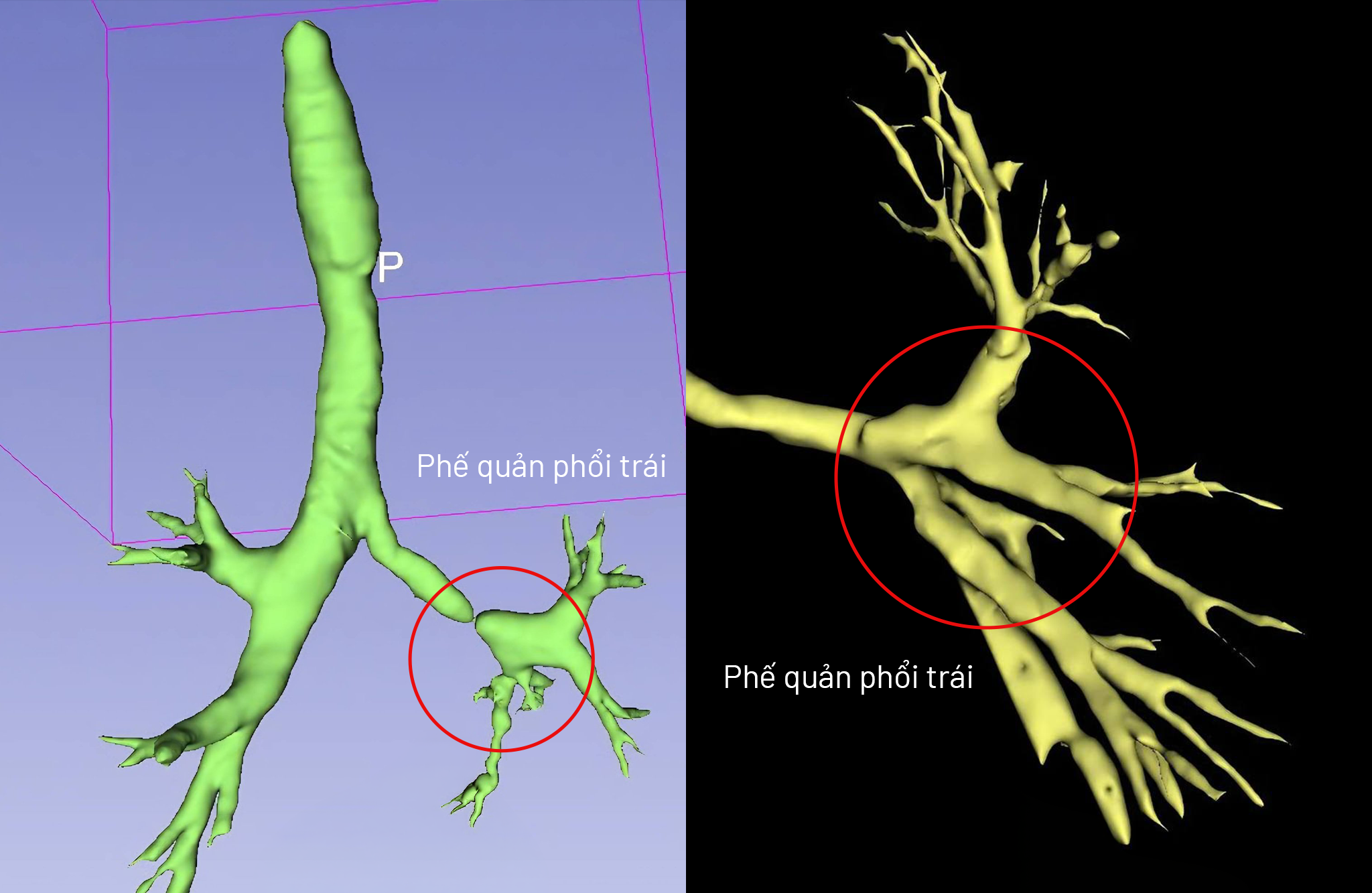 |
3D CT scans before surgery (left) and after surgery (right) show the narrowed bronchial segment was almost completely corrected. *Photo: Tam Anh General Hospital* |
Associate Professor Vinh explained that the patient's lower lobe bronchus was severely damaged, and performing a lobectomy of the upper lobe, as in conventional techniques, would significantly impair lung function. The primary challenge for the anesthesia team was maintaining blood oxygen levels when the patient's airway was as narrow as a toothpick tip. Throughout the surgery, doctors meticulously adjusted every one milliliter of gas delivered to the lung to avoid increasing pressure in the already fibrotic airway, while ensuring the lung did not completely collapse.
Due to the long-standing collapsed left lung and chronic oxygen deficiency, the patient's heart had to operate under extreme conditions, increasing the risk of arrhythmia or sudden cardiac arrest on the operating table. The team prepared various cardiac support and vasopressor options. Concurrently, Associate Professor Vinh transversely cut the middle of the narrowed bronchial segment, then longitudinally incised both ends of the cut tube in symmetrical directions. These two sections were then slid over each other and sutured, maximizing the airway diameter and preventing lung hypoxia.
The surgery was successful after more than 5 hours; the bronchus was widened, and the lung was completely preserved. Aye resumed normal activities and work after her recovery.
 |
Associate Professor Vinh (center) with the surgical team performing bronchial reconstruction for the patient. *Photo: Tam Anh General Hospital* |
Doctors anticipated Aye would require approximately one month of intensive care unit (ICU) treatment post-surgery due to the complex damage. However, thanks to effective intraoperative control, intensive resuscitation, and aggressive postoperative care, she recovered quickly and was discharged after 5 days. With stable vital signs and regular breathing, Aye experienced no chest pain or shortness of breath on exertion.
 |
Associate Professor Vinh examines the patient 3 days after surgery. *Photo: Tam Anh General Hospital* |
Bronchial stenosis is common in individuals with a history of tuberculosis. If not surgically treated promptly, patients risk irreversible lung damage, respiratory failure, and life-threatening complications. Associate Professor Vinh advises that those with a history of pulmonary tuberculosis should not be complacent about respiratory symptoms after treatment. If symptoms such as persistent shortness of breath, wheezing, or chest pain during activity occur, patients should seek immediate medical examination.
Bao Anh
*Patient's name has been changed
| Readers can submit questions about respiratory diseases here for doctors to answer. |









