Beyond breast development, Huyen showed no other signs of puberty. Doctor Do Tien Son, head of Pediatrics at Tam Anh General Hospital Hanoi, noted the child's mammary glands had developed to Tanner stage B3, a phase characterized by rapid and clear appearance of breast tissue. The left ovary contained a large cyst, approximately 43x37x29 mm, with thin walls and clear fluid, containing a smaller cyst inside. The lesion was classified as ORADS 2, indicating a low risk of malignancy. MRI confirmed the left ovarian cyst was benign. X-ray results showed no increase in bone age, which currently matched the child's chronological age.
Estradiol, a female sex hormone, was significantly elevated, while luteinizing hormone (LH) secreted by the pituitary gland remained low. Doctor Son suspected peripheral precocious puberty caused by a functional ovarian cyst secreting estrogen, rather than central precocious puberty where the central nervous system's regulatory axis triggers puberty. Functional ovarian cysts are fluid-filled sacs that form in the ovaries, linked to endocrine activity. Most cases are benign and can resolve spontaneously over time, according to Doctor Son.
The specific cause is often undetermined in most cases. However, doctors ruled out rare causes such as ovarian granulosa cell tumors (tumors that can secrete hormones) or McCune-Albright syndrome, a genetic disorder causing precocious puberty alongside skin pigmentation abnormalities and bone lesions. Currently, Huyen does not exhibit typical symptoms of these conditions but requires regular monitoring.
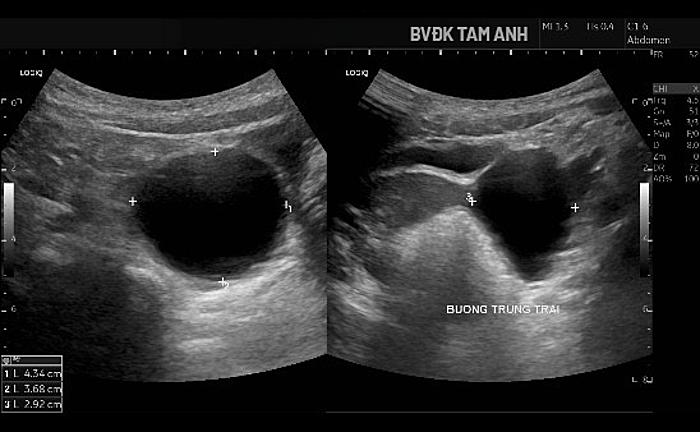 |
Ultrasound image showing the enlarged ovarian cyst. Photo: Tam Anh General Hospital |
Doctor Son explained that when ovarian cysts secrete estrogen, children may exhibit signs of puberty like breast development or vaginal bleeding. A small percentage of children could progress to central precocious puberty if the pubertal axis is activated after prolonged exposure to sex hormones, potentially leading to rapid bone age advancement and affecting adult height. Early bodily changes also impact a child's psychological well-being. Furthermore, children with enlarged ovarian cysts face a risk of acute complications such as ovarian torsion or cyst rupture, requiring emergency treatment.
Doctors scheduled Huyen for a follow-up examination after two weeks to assess the cyst's size trend. Subsequently, she will undergo regular monitoring every three months to review changes in cyst size, breast development, height, bone age, and growth rate.
During the follow-up visit, Huyen's signs of precocious puberty significantly decreased, hormone levels dropped, and the functional ovarian cyst was regressing, with its size reduced by approximately 20%. Doctors will continue to closely monitor the condition's impact on growth and bone age.
Doctors thoroughly explained potential scenarios to the family, including early vaginal bleeding, the risk of progression to central puberty, or underlying genetic-endocrine factors. The child should be taken to the hospital immediately if experiencing severe abdominal pain, vomiting, fever, abdominal distension, unusual fussiness, or vaginal bleeding, as these could indicate ovarian torsion, cyst rupture, or other acute issues.
Doctor Son recommends that children showing signs of precocious puberty (breast development, pubic hair growth, or rapid height increase before 8 years old in girls and 9 years old in boys) undergo specialist examination to determine the cause. Parents should not administer hormone medication without medical guidance; instead, they should closely monitor their child's development and encourage a healthy lifestyle.
Trinh Mai
| Readers can submit questions about neonatal pediatrics here for doctors to answer. |