Master of Science, Doctor of Medicine, Second Degree Specialist Lam Thien Kim, from the Department of Pediatric Surgery at Tam Anh General Hospital, TP HCM, reported that the pediatric patient experienced intermittent abdominal pain, fatigue, and an unusual mass in the right upper abdomen. Ultrasound results confirmed acute ileocecal intussusception, with the intussuscepted mass located below the liver, measuring approximately 37 mm in diameter and 81 mm in length. Blood supply to the bowel wall within the intussuscepted segment was still intact, while the small bowel loops in the left abdomen were dilated and distended with gas.
Doctor Kim diagnosed Tung with acute intussusception and immediately ordered an emergency reduction to avert the risk of intestinal ischemia and necrosis.
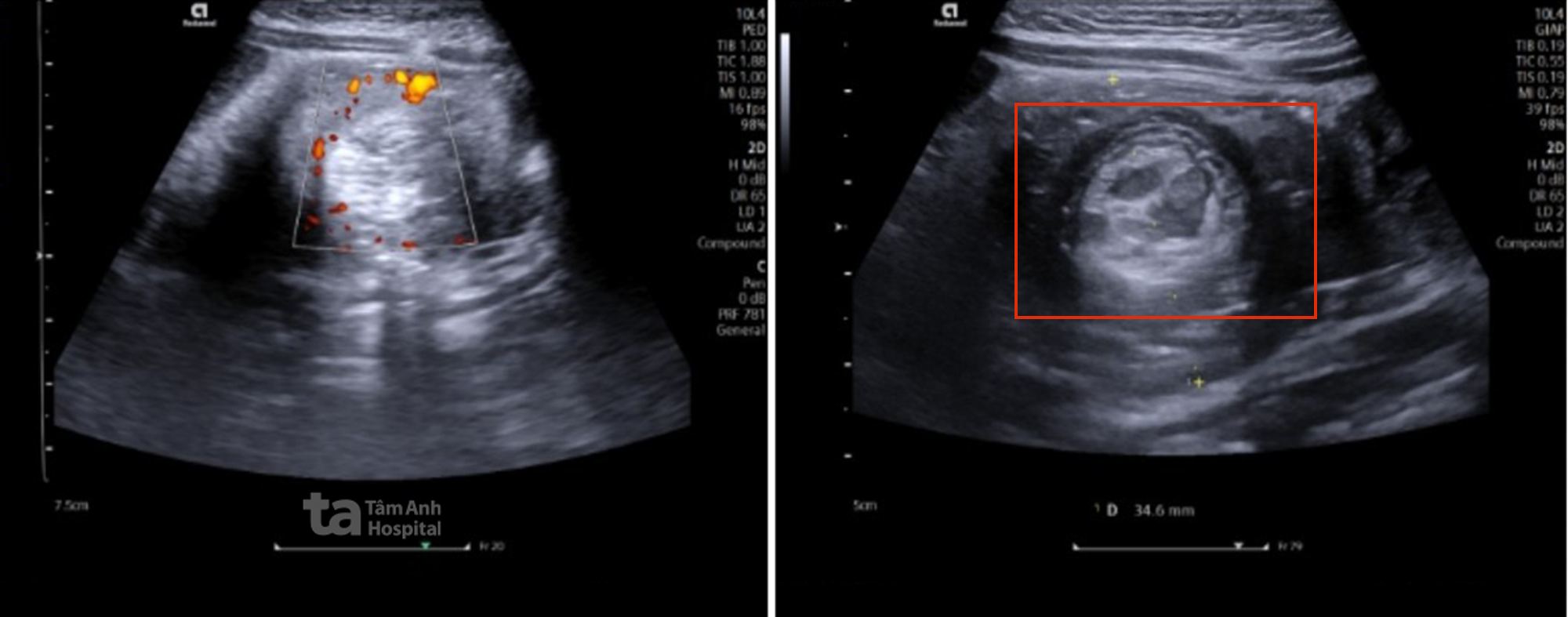 |
Ultrasound image showing the pediatric patient with acute intussusception. Photo: Tam Anh General Hospital |
Following general anesthesia, Doctor Kim inserted a gastric tube and an anal tube, then inflated the colon with air at a pressure of 90-110 mmHg in three consecutive attempts to reduce the intussusception.
 |
The medical team inflates the colon to reduce the intussusception for the pediatric patient. Photo: Tam Anh General Hospital |
After the procedure, the boy received fluid resuscitation and antibiotics. His health stabilized, and he was discharged.
According to Doctor Kim, air enema reduction for young children requires general anesthesia to ensure safety and enhance the procedure's effectiveness. When doctors inflate the colon to push the intussuscepted segment back to its normal position, it can cause pain, leading to crying and excessive movement in children. If the child does not remain still, the air pressure can become unstable, reducing the effectiveness of the reduction and increasing the risk of complications. Anesthesia helps the child sleep deeply, remain pain-free, and maintain a stable airway, assisting doctors in precisely controlling the air pressure during the intervention.
Intussusception is a condition where one segment of the intestine slides into an adjacent segment, compressing blood vessels supplying the bowel and causing an obstruction of intestinal flow. This condition is most common in children aged six months to 5 years.
Doctor Kim stated that the cause of intussusception in children is often unclear. It may be linked to increased bowel motility following gastrointestinal or respiratory viral infections, lymphoid tissue hypertrophy in the intestine, or abnormalities such as polyps or Meckel's diverticulum.
In the initial stage of the disease, children may experience intermittent abdominal pain, fussiness, or mild vomiting, which can be mistaken for a digestive disorder. This can lead to bloody stools in later stages. If not treated promptly, children risk intestinal ischemia, necrosis, and severe infection. However, many cases present with unclear abdominal pain or no bloody stools, leading to delayed hospital admission. Doctors advise parents to monitor for unusual symptoms in children, especially after episodes of digestive upset or viral infections.
If detected and reduced within the initial 24 hours of symptom onset, most cases can be treated with air enema, avoiding the need for surgery.
Minh Tam
* Patient's name has been changed
| Readers can send questions about pediatric diseases here to receive answers from doctors |