Mr. Hung's symptoms appeared about one month ago, including occasional dull pain in the upper abdomen. The pain worsened when lying on his back and eased when sitting in a forward-leaning position, prompting him to visit Tam Anh General Hospital Ho Chi Minh City for examination.
An abdominal ultrasound revealed a hypoechoic mass measuring approximately 70 mm in the head of the pancreas, accompanied by surrounding tissue edema. Smaller lesions were also noted in the body and tail of the pancreas. A subsequent abdominal CT scan confirmed a lesion in the pancreatic head, causing dilation of both intrahepatic and extrahepatic bile ducts, leading doctors to suspect malignancy. The tumor had indistinct margins with the D2 segment of the duodenum. The gallbladder was distended and contained gallstones and biliary sludge, with several lymph nodes observed around the pancreatic head and porta hepatis.
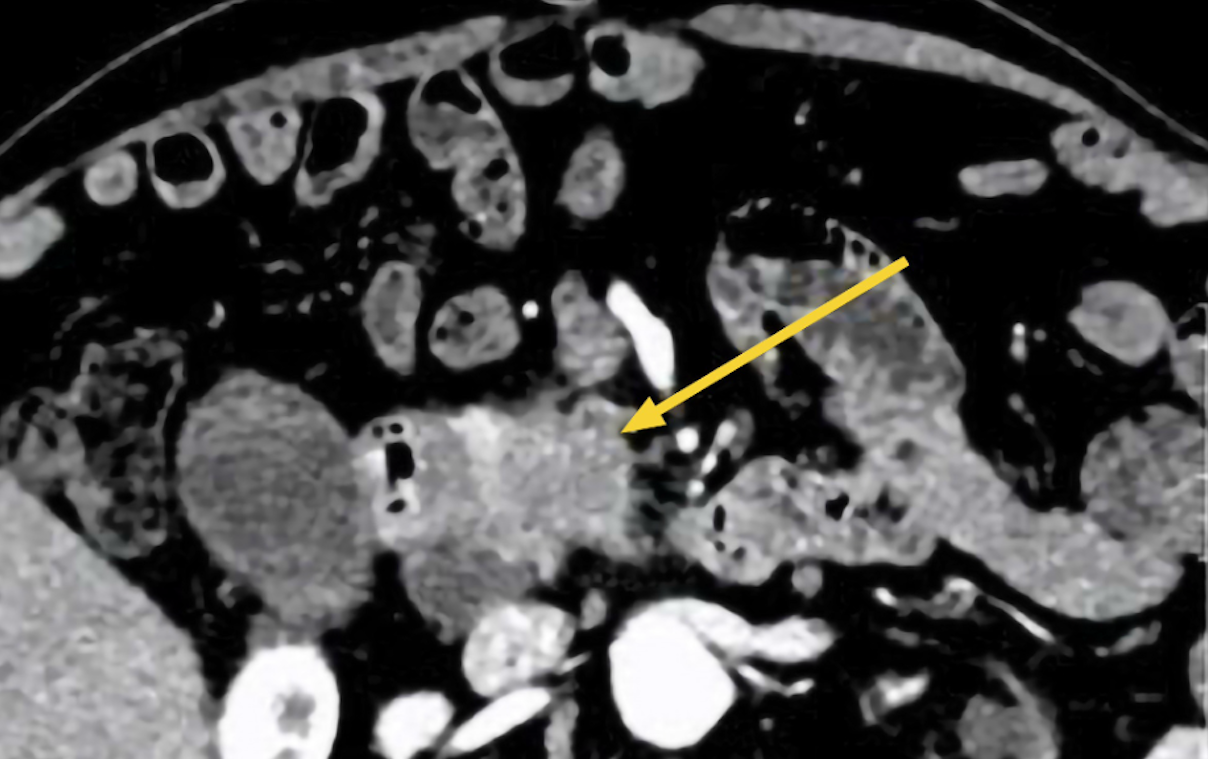 |
CT scan showing Mr. Hung's pancreatic head lesion (yellow arrow). *Photo: Tam Anh General Hospital* |
Doctor Do Minh Hung, Director of the Center for Endoscopy and Endoscopic Gastrointestinal Surgery at Tam Anh General Hospital Ho Chi Minh City, diagnosed Mr. Hung with stage two pancreatic ductal adenocarcinoma. The tumor had metastasized to one lymph node near the pancreatic head and showed signs of vascular and perineural invasion.
The patient underwent biliary drainage to alleviate jaundice and reduce infection, stabilizing his health. Subsequently, doctors convened a consultation and recommended a robotic-assisted laparoscopic pancreaticoduodenectomy (Whipple procedure) for Mr. Hung using the Da Vinci Xi robot, aiming for complete tumor removal while minimizing invasiveness and metastasis.
According to Doctor Hung, the pancreatic head is rich in vital blood vessels, including the superior mesenteric artery and portal vein, making the surgery particularly challenging. Additionally, the patient's existing comorbidities, such as diabetes, hypertension, and coronary artery disease, could increase the risk of bleeding and complications during and after the operation.
During the surgery, doctors removed the pancreatic head, duodenum, a portion of the jejunum, the common bile duct, the gallbladder, and associated lymph nodes. Digestive continuity was then re-established through anastomoses connecting the pancreas, bile duct, and small intestine. Thanks to the robot's flexible arms, the team precisely dissected the tumor and lymph nodes in the deep, confined area, which helped reduce the risk of cancer recurrence, before performing the pancreatic-intestinal anastomosis.
After the 10-hour surgery, Mr. Hung recovered well, with a dry incision, minimal pain, and the ability to perform light movements after one day. The patient began eating again under medical guidance and was discharged on the 10th day.
Pathology results indicated that the surgical margins were clear of cancer cells. However, due to lymph node metastasis, Mr. Hung will continue to receive follow-up care and adjuvant therapy.
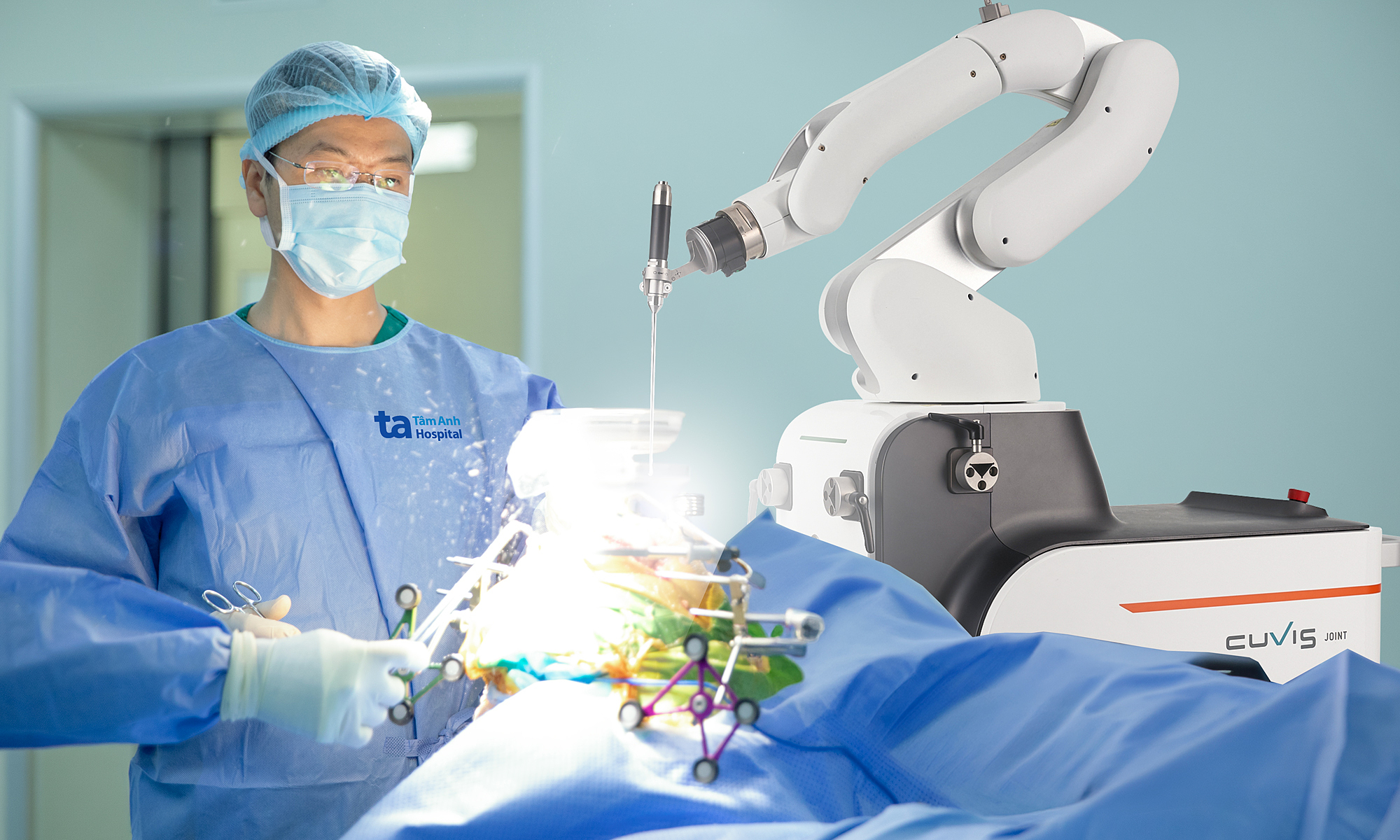
 |
Surgical team performing a laparoscopic pancreaticoduodenectomy for Mr. Hung. *Photo: Tam Anh General Hospital* |
Pancreatic cancer progresses rapidly, with initial symptoms often vague and challenging to detect in early stages. As the pancreas is located deep within the abdomen, small tumors are difficult to identify through routine examinations. Distinct symptoms typically emerge only when the tumor grows large enough to obstruct the bile duct or destroy pancreatic tissue.
Doctor Hung advises everyone to undergo regular health check-ups at least once a year. If unusual symptoms appear, such as dull upper abdominal pain radiating to the back, increased pain when lying flat, jaundice, yellow eyes, or unexplained weight loss, it is crucial to seek medical attention for timely diagnosis and treatment.
Quyen Phan
*Patient's name has been changed
| Readers can submit questions about digestive diseases here for doctors to answer |