

The large intestine in adults typically measures 120-150 cm. Master, Doctor Nguyen Thanh Bien, from the Center for Endoscopy and Endoscopic Digestive Surgery, reported removing over 60 cm of a patient's sigmoid colon due to severe volvulus and distension. This resection meant the patient lost about 50% of his large intestine, potentially leading to digestive changes like indigestion, bloating, and infrequent bowel movements. He will require an easily digestible diet and regular follow-ups to monitor his condition and prevent complications.
Previously, Minh suffered from constipation, which was treated with medication and a rectal tube. Three months later, his abdomen became severely distended, causing shortness of breath, abdominal pain, and an inability to eat, requiring nutritional infusions. A 1975-slice CT scan at Tam Anh General Hospital revealed sigmoid colon volvulus (the final segment of the large intestine), with the mesentery blood vessels and the sigmoid colon loop twisted, measuring 20 cm in diameter—nearly 7 times larger than normal. The intestinal lumen was filled with gas and waste, and the intestinal wall was thin.
Doctor Bien diagnosed Minh with sigmoid colon volvulus, which obstructed intestinal flow and blood supply, leading to intestinal obstruction. The doctor recommended surgery to prevent stool and fluid leakage from the intestine into the abdominal cavity, which could cause complications.
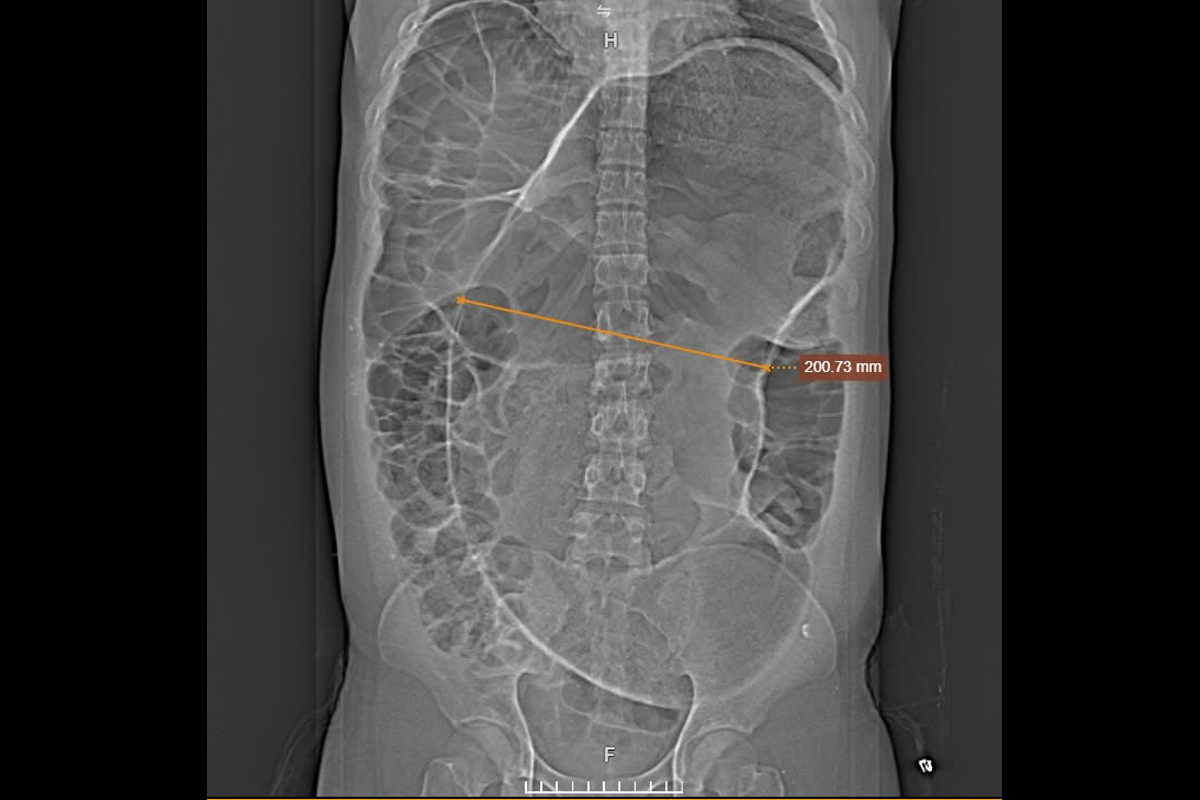 |
Computed tomography showed the distended colon segment (yellow arrow). *Photo: Tam Anh General Hospital* |
Doctor Bien described the surgery as challenging because the patient's sigmoid colon was massively distended with an edematous wall. His abdomen was severely bloated and congested, with almost no peristalsis. This condition prevented laparoscopic surgery, as carbon dioxide could not be insufflated to create a surgical field, necessitating an open procedure.
Doctors resected the twisted sigmoid colon segment and created a temporary colostomy in the patient's left flank. The intestine was greatly distended and edematous, posing a high risk of leakage, making immediate re-anastomosis during the surgery impossible. After about three months, once his general condition stabilizes, the patient will undergo surgery to close the colostomy.
Doctors resecting a segment of Minh's colon. *Photo: Tam Anh General Hospital* |
Sigmoid colon volvulus is a surgical emergency requiring prompt intervention. It affects all ages, primarily caused by a long, loose sigmoid mesentery (redundant colon) that allows excessive bowel mobility, making it prone to twisting. Risk factors include individuals over 50, especially bedridden patients with reduced bowel motility or a history of chronic constipation. Stool impaction can distend the sigmoid colon, increasing volvulus risk. Mental illness and prior abdominal surgery, which can form adhesive bands, are also contributing factors.
If detected early, when the intestine is edematous, distended, and only slightly twisted, doctors can perform a flexible endoscopic detorsion with a gentle procedure and low risk. Individuals experiencing abdominal pain and distension, nausea, and inability to pass gas or stool should seek medical attention for diagnosis.
Quyen Phan









