Mr. Chinh was admitted to Tam Anh General Hospital Hanoi in a deep coma, with a Glasgow Coma Scale (GCS) score of 7 (a healthy individual scores 15), and dangerously high blood pressure at 204/117 mmHg. A CT scan of his brain revealed a hematoma measuring 32x37 mm. This lesion caused a mass effect, displacing the midline 8 mm to the right, and had ruptured into the left lateral ventricle, resulting in bilateral intraventricular hemorrhage.
Master of Science, Doctor Le Van Ngan from the Department of Neurosurgery and Spine noted that patients admitted with a GCS score below 9 and a blood clot size of 60 ml or more typically face a mortality rate of nearly 90%. Mr. Chinh's condition was identified as a left thalamic intracerebral hemorrhage caused by hypertension. Blood pressure exceeding 140/90 mmHg damages the intricate network of blood vessels supplying the brain, leading to their rupture and subsequent hemorrhage.
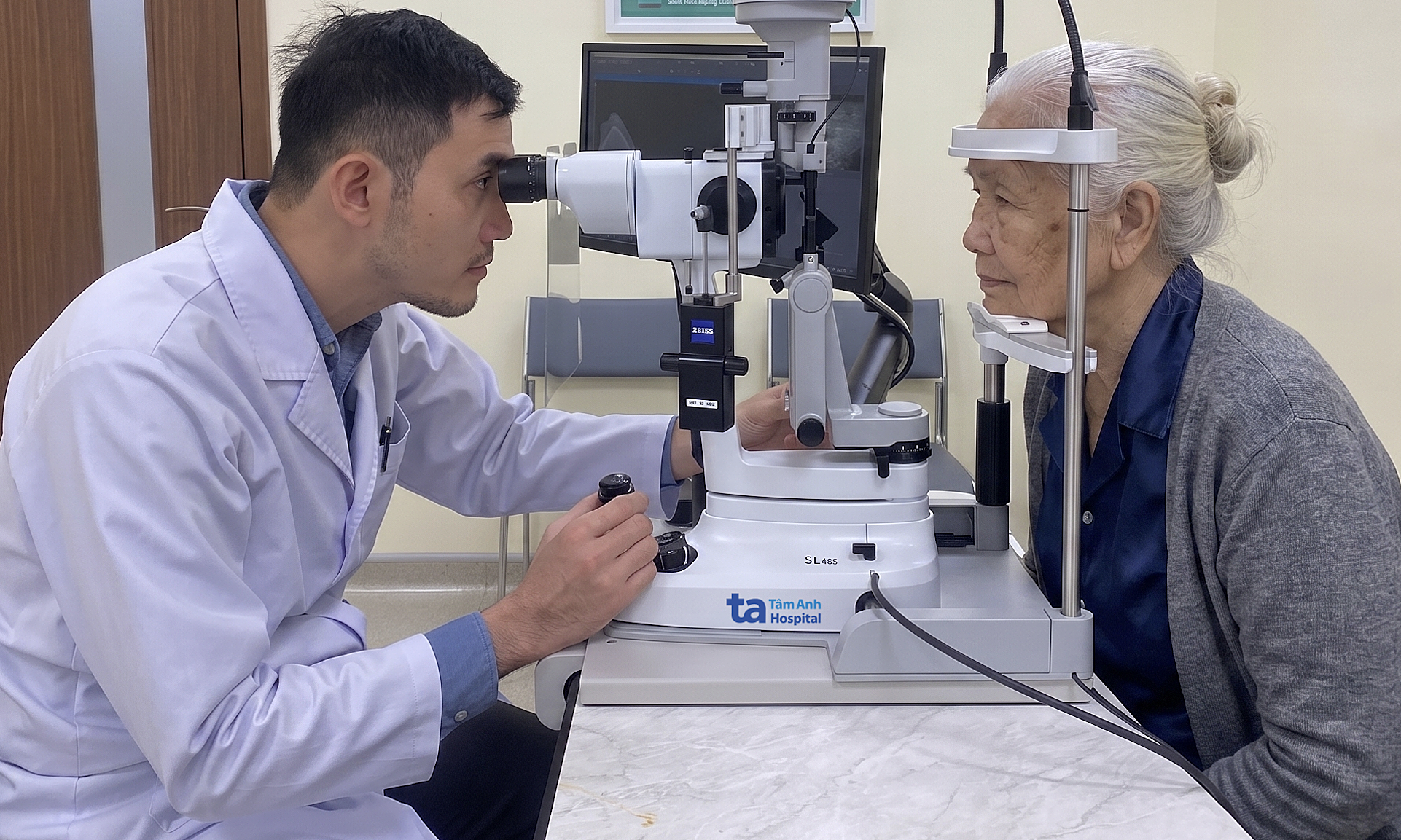
The surgical team removes an intracranial hematoma from the patient. *Photo: Tam Anh General Hospital* |
The patient's blood pressure was immediately brought under control, and mechanical ventilation was initiated. Concurrently, preparations were made for emergency craniotomy to remove the intracranial hematoma. Doctors strategically placed a ventricular catheter to effectively manage the elevated intracranial pressure.
After precise anatomical localization of the ventricle, the catheter was carefully inserted to remove the accumulated blood clot and drain cerebrospinal fluid, thereby reducing intracranial pressure. This sophisticated system continuously monitors intracranial pressure, providing crucial real-time data that allows doctors to fine-tune resuscitation strategies, control cerebral edema, and optimize cerebral perfusion following surgery.
Following the surgery, Mr. Chinh remained in a deep coma, primarily due to the late detection of the cerebral hemorrhage and the delay in his arrival at the emergency room. He received mechanical ventilation support for approximately one week before being successfully weaned off the ventilator and transferred back to the Department of Neurosurgery and Spine.
Once off the ventilator, Mr. Chinh underwent comprehensive medical treatment, including antibiotics, medication to support brain function, and early physical rehabilitation. These interventions aimed to improve his muscle strength and mitigate common complications such as pneumonia from prolonged bed rest and pressure ulcers. Simultaneously, strict blood pressure control was maintained to prevent any recurrence of the cerebral hemorrhage.
Currently, Mr. Chinh is fully conscious. However, he continues to experience right-sided weakness, with muscle strength rated 4/5, exhibits slurred speech, and requires ongoing assistance for daily care.
Hypertensive cerebral hemorrhage is a dangerous neurological condition that can lead to severe long-term sequelae or even death if not managed promptly. Patients with a history of cerebral hemorrhage must undergo vigilant monitoring and rigorous blood pressure control, as the risk of recurrence is high, and subsequent events often present with greater severity than the initial one.
Hang Tran